Look, nobody likes getting that phone call. You know the one. A surgeon calls the procurement office, clearly frustrated, because an implant failed in a patient six months post-op. A plate snapped right across the screw hole. Now the patient needs a revision surgery, the hospital is looking at potential liability, and you’re left wondering if you bought a bad batch of hardware.
If you’re sourcing implants or you’re the one putting them into patients, you already know the stakes are incredibly high. But I’ll tell you right now, most people misunderstand why these plates actually break. It’s rarely a massive, sudden impact that snaps the metal. It’s almost always material fatigue.
Let’s strip away the marketing fluff. We need to talk about the reality of orthopedic plate lifespan, how the metal actually behaves inside the human body, and why picking the cheapest option on your spreadsheet is playing a dangerous game with patient safety.
Why Plates Break: It’s Not What You Think
I’ve spent years looking at failed implants and talking to the folks who make them and the doctors who use them. A massive misconception in the orthopedic market is that a strong plate is a plate that won’t break. Wrong.
Strength and fatigue resistance are two totally different animals.
Think about a paperclip. You can’t pull a paperclip apart with your bare hands no matter how hard you yank on it. It has high tensile strength. But if you bend it back and forth slightly about twenty times? It snaps easily. That’s material fatigue.
When a patient has a comminuted femur fracture and the surgeon bridges the gap with a locking plate, the bone isn’t sharing the load right away. The plate takes all the force. Every single time that patient takes a step, the plate bends just a microscopic amount.
Let’s do some quick, ugly math. No fancy textbook formatting, just real numbers.
Average person takes about 1 to 2 million steps a year.
When walking, the force on the femur is roughly 2.5 times body weight.
For an 80kg (176 lb) patient, that’s 200kg of force pushing down on that leg.
So the plate is getting slightly bent with 200kg of force, a million times a year. If the bone takes too long to heal (delayed union or non-union), the plate is forced to endure this cyclic loading way past its intended design. Eventually, a microscopic crack forms. Then it grows. Then, bang. The plate fractures.
This is why understanding bone plate fatigue strength is literally the most critical part of evaluating an implant. It’s the only thing standing between your patient and a second trip to the operating room.


1.5mm Mini Condylar Locking Plate | Titanium Hand & Finger Fracture Implants | OrthoPro
The 1.5mm Mini Condylar Locking Plate is precision-engineered for the fixation of intra-articular and condylar fractures in phalanges and metacarpals. Featuring a low-profile anatomical design, this mini condylar locking plate ensures stable reconstruction of the joint surface while minimizing soft tissue irritation. OrthoPro supplies high-quality 1.5mm locking plates to global orthopedic distributors.
The Big Material Debate: Why I’m Biased
I’ll just say it out loud, and some old-school surgeons might get mad at me for this: hospitals that still push heavy stainless steel plates for lower limb load-bearing fractures are making a mistake.
Yeah, I know 316L stainless steel is cheap. I know it’s what a lot of older docs trained on. It bends nicely in the OR when you’re trying to contour it to the bone. But stainless steel is simply too stiff, and its fatigue properties in a corrosive saltwater enviornment (which is basically what the human body is) are completely inferior to titanium.
When a plate is too stiff, it causes “stress shielding.” The bone gets lazy because the plate is doing all the work. Bone needs stress to heal and grow strong (Wolff’s Law). If the bone doesn’t heal, the plate keeps taking all the weight indefinitely. And remember the paperclip? No metal can take cyclic loading forever if the stress is too high.
This is where medical grade titanium comes in. Specifically, Ti-6Al-4V ELI (Extra Low Interstitials).
Titanium has a lower modulus of elasticity than stainless steel. That means it’s more flexible. It flexes closer to the natural flexibility of human bone, which promotes callus formation and faster bone healing. The faster the bone heals, the faster the bone starts sharing the load with the plate, which drastically extends the orthopedic plate lifespan.
Here is a quick look at the raw numbers. I threw this together so you can see the difference:
| Material Property | 316L Stainless Steel | Pure Titanium (CP Ti Grade 4) | Ti-6Al-4V ELI (Titanium Alloy) |
|---|---|---|---|
| Tensile Strength (MPa) | ~600 | ~680 | ~900+ |
| Yield Strength (MPa) | ~300 | ~480 | ~800+ |
| Fatigue Limit (MPa at 10^7 cycles) | ~250 | ~300 | ~500+ |
| Elastic Modulus (GPa) | 200 (Very stiff) | 105 (Closer to bone) | 110 (Closer to bone) |
Data sourced from standard ASTM implant material specifications.
Look at that Fatigue Limit row. The titanium alloy can handle double the repeated stress before cracking compared to standard stainless steel. If you are a buyer trying to minimize risk, why would you ever skimp on the material?
The Dirty Little Secret of Manufacturing
Okay, so you bought a titanium plate. You’re safe, right?
Not even close.
I’ve seen absolute garbage titanium plates on the market. The raw material might be certified ASTM F136 titanium, but the way the factory actually made the plate ruined it.
You see, material fatigue always starts at a “stress riser.” A stress riser is any sharp corner, deep scratch, or rough edge on the metal. When the plate bends, all the force concentrates right at that tiny defect.
Bad Machining = Dead Plates
If a factory is trying to cut costs, they might run their CNC milling machines too fast, or they might use dull cutting tools to save money on tooling replacements. When a dull tool cuts titanium, it tears the metal rather than slicing it cleanly. This leaves microscopic gouges and tears on the surface of the plate, especially inside the screw holes.
You can’t see them with your naked eye. But under a microscope, those tear marks are massive canyons just waiting to turn into cracks. The moment the patient starts walking, the crack initiates at that bad machining mark.
Surface Treatments Matter
Good factories—the kind of places making implants for brands like OrthoPro—spend an insane amount of time on surface finishing.
They use specialized tumbling and polishing processes to smooth out every single microscopic edge. Sometimes they use a process called shot peening. This is where they blast the surface of the metal with tiny ceramic or glass beads. It sounds destructive, but it actually compresses the outer layer of the titanium.
Here’s the simple science: cracks can only open up if the metal is being pulled apart (tension). If the surface of the metal is permanently compressed by shot peening, the walking forces have to overcome that compression before they can even start pulling the metal apart. It’s a brilliant way to massively increase bone plate fatigue strength without changing the design at all.
Color anodizing is another thing people misunderstand. They think the plates are colored blue or green or gold just to look pretty or to help the surgical tech match the right screws (which it does). But anodizing also creates a thick titanium dioxide layer on the surface that improves corrosion resistance and reduces the chance of galling (cold welding) between the screw head and the plate. Less friction, less wear, longer lifespan.
Real Talk: A Sourcing Nightmare I Watched Unfold
I want to share a story about a hospital procurement director I know. I’ll keep his name and the hospital anonymous, but he was working for a large private healthcare group in South America.
A few years ago, his finance department came down hard on his budget. They demanded a 15% reduction in trauma implant costs across the board. So, he found a new overseas supplier. The supplier showed him the raw material certificates—yes, it was real medical grade titanium. The price was incredibly low. He signed the contract and felt like a hero.
Six months later, the nightmare started.
Over a four-week period, they had three separate patients come back to the ER with broken distal femur locking plates. Three. In one month. The surgeons were absolutely furious. The hospital had to cover the cost of the revision surgeries, the new implants, the extended hospital stays, and they narrowly avoided a massive lawsuit from one of the patients.
When they sent the broken plates out for independent metallurgical testing, the results were shocking. The raw material was fine. But the machining was atrocious. The supplier hadn’t chamfered the locking threads properly, and there were massive burrs and micro-cracks left behind by cheap cutting tools. The fatigue strength was practically non-existent.
The procurement director had to throw away thousands of dollars in inventory and immediately switch back to a premium supplier. The “savings” from the cheap plates ended up costing the hospital easily ten times more in the end.
The lesson here? Never buy off price and raw material alone. You have to understand the manufacturing quality.
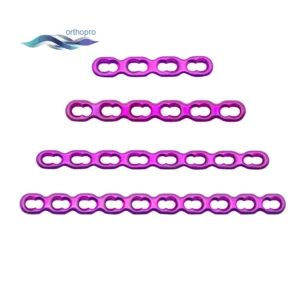


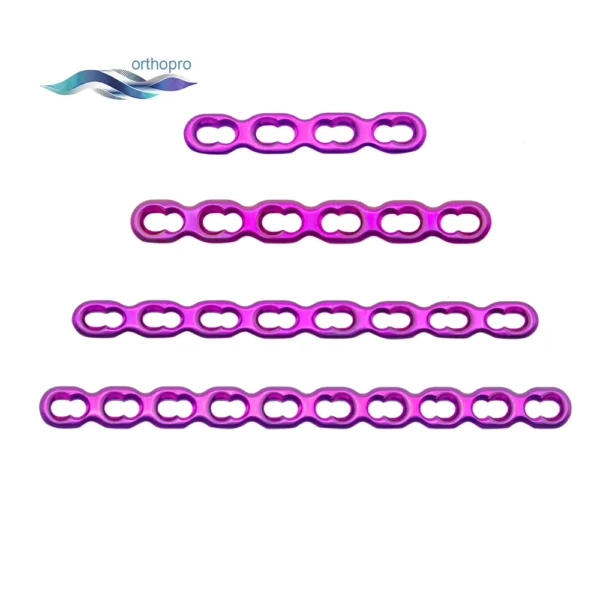

2.0mm Mini Adaptation Locking Plate | Titanium CMF & Hand Surgery Implants | OrthoPro
The 2.0mm Mini Adaptation Locking Plate is engineered to provide versatile fixation for fractures in the craniomaxillofacial (CMF) region and hand. Featuring a malleable design, this mini adaptation locking plate allows for precise 3D contouring to fit irregular bone surfaces. OrthoPro supplies these high-performance 2.0mm locking plates to global distributors, ensuring superior stability for complex reconstructive surgery
The Math Behind the Break (Keeping it simple)
If you really want to nerd out on how engineers calculate this stuff, there are a few basic principles you should know. Don’t worry, I won’t use unreadable LaTeX formatting.
Basically, the stress on a plate in the body acts like a beam bending under a load.
The basic formula for bending stress is:
Stress (S) = (Bending Moment * distance from the center) / Moment of Inertia
Bending Moment is basically the patient’s weight multiplied by the distance from the fracture gap.
Moment of Inertia is about the shape of the plate. A thicker plate has a much higher moment of inertia, meaning it handles stress much better.
But you can’t just make the plate two inches thick, because it won’t fit under the patient’s skin and it will cause massive stress shielding. So engineers have to find the perfect balance. They design plates that are thick exactly where the fracture usually happens, and thinner at the ends.
Then they test it.
Fatigue Testing Data You Should Actually Ask For
If you are evaluating a new trauma plate supplier, do not just ask for a brochure. Ask for their ASTM F382 fatigue test report.
ASTM F382 is the standard specification and test method for metallic bone plates. The lab takes the plate, puts it into a machine that simulates a bone gap, and bends it repeatedly.
They generate something called an S-N curve (Stress vs. Number of cycles).
They apply a high stress, and the plate breaks at maybe 10,000 cycles.
They lower the stress, and it breaks at 100,000 cycles.
They keep lowering the stress until they find the “Runout” limit. This is the stress level where the plate survives 1,000,000 cycles without breaking.
One million cycles is the magic number in orthopedics. It represents roughly a year of walking. If the bone hasn’t healed in a year, you have bigger clinical problems than the plate.
If a supplier hems and haws and makes excuses when you ask for their fatigue testing data, run away. It means they are guessing. Serious manufacturers know their fatigue numbers by heart because they test every single design iteration.
How Surgeon Technique Ruins Good Plates
I have to defend the manufacturers for a second here. Sometimes, the plate breaks and it is 100% the surgeon’s fault.
Even the highest quality medical grade titanium plate will fail if it is abused in the operating room. Titanium is notoriously sensitive to “notch sensitivity.”
When a surgeon uses plate benders to contour a flat plate to match the curve of a pelvis or a tibia, they have to be careful. If they use the wrong bending irons, or if they bend the plate back and forth multiple times to get the shape right, they are drastically reducing the orthopedic plate lifespan. Bending it back and forth work-hardens the titanium and creates microscopic stress risers before the plate is even screwed in.
Also, if a surgeon leaves an empty screw hole right over the fracture gap (which is the point of maximum bending stress), they are asking for trouble. An empty hole reduces the cross-sectional area of the metal, meaning the stress skyrockets right at that weak point.
Good surgical technique involves getting the contour right the first time, using plates that are pre-contoured from the factory whenever possible, and placing screws strategically to distribute the load.
Final Thoughts Before the FAQ
Procuring orthopedic trauma implants is a massive responsibility. You are buying the temporary scaffolding that holds a human’s life together while their body heals.
Understanding material fatigue isn’t just an engineering exercise; it is risk management. It’s about knowing that Ti-6Al-4V is better than stainless steel for load-bearing fatigue. It’s about knowing that a smooth, perfectly machined surface finish prevents crack initiation. And it’s about partnering with manufacturers who actually understand the biomechanics of what they are making.
Quick FAQ: Your Questions Answered
Q: How long is a standard orthopedic plate lifespan supposed to be?
Honestly, it’s designed to last until the bone heals, which is usually 3 to 6 months. Once the bone is fully consolidated, the plate isn’t really doing much mechanical work anymore. In theory, a titanium plate can stay in the body forever without degrading, but its active working lifespan is focused on that first million load cycles.
Q: Does removing the plate early prevent fatigue failure?
Surgeons generally don’t reccomend routine plate removal anymore unless the hardware is causing soft tissue irritation or infection. The risks of a second surgery (nerve damage, infection, re-fracture) usually outweigh the risk of leaving a healed plate in place. Once the bone is healed, fatigue failure of the plate is extremely rare because the bone is taking the weight.
Q: Is stainless steel ever a better choice than titanium?
I’m tough on stainless steel, but it does have a place. For upper extremity fractures (like the wrist/distal radius) where the weight-bearing loads are minimal, stainless steel works fine and is cost-effective. But for femurs and tibias? I strongly advise sticking to titanium alloys.
Q: Can you tell if a plate has good fatigue strength just by looking at it?
Nope. You might see obvious rough machining marks if it’s truly terrible, but the micro-cracks that cause failure are invisible to the naked eye. You must rely on the manufacturer’s ASTM F382 test reports and their quality control documentation.
Let’s Get Real About Your Next Order
If you are tired of losing sleep over implant quality, or if your current supplier is treating your technical questions like an annoyance, it’s time to make a change.
You need implants that are engineered for the real world—implants where the surface finish, the material grade, and the machining tolerances are obsessed over. That’s exactly what the team at OrthoPro does. We don’t just sell metal; we sell the confidence that when that patient walks out of the hospitel, that plate is going to hold.
Don’t wait for a catastrophic failure in the OR to re-evaluate your supply chain.
Check out our full line of rigorously tested implants, or better yet, let’s talk about your specific needs and pricing. Drop us a message right now through our contact page or email us directly at info@orthopro.mx. We can provide the testing data, the material certs, and the competitive quotes you need to make a smart, safe decision for your patients.





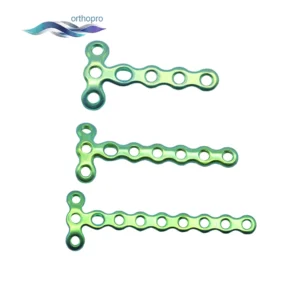
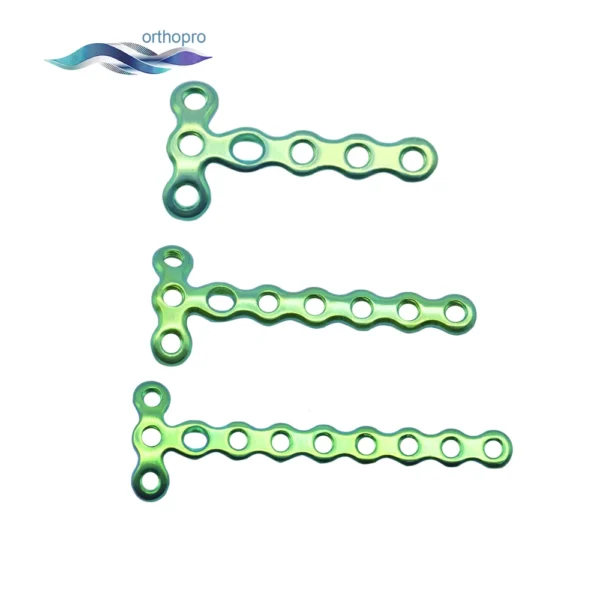
1.5mm Mini Y Locking Plate | Titanium Hand & Foot Fracture Implants | OrthoPro
The 1.5mm Mini Y Locking Plate is expertly designed for the fixation of peri-articular fractures in phalanges and metacarpals. Featuring a specialized Y-geometry, this mini Y locking plate allows for multi-point fixation near joints while minimizing soft tissue irritation. OrthoPro supplies these high-precision 1.5mm locking plates to global orthopedic distributors, ensuring superior stability for complex small bone trauma.
